
Coronary Artery Disease (Part 1)
The more you know about the underwriting process, the better equipped you will be to address the questions that arise in underwriting life insurance protection today. Your FIELD UNDERWRITING expertise is even more important now in this age of electronic applications and Drop-Tickets. Your clients have high expectations and depend upon your knowledge to direct their unique medical and financial circumstances to the right carrier. The Underwriting Team at AgencyONE is here to address all your questions and concerns…and point you in the right direction.
This week’s ONE Idea on Coronary Artery Disease (CAD) is the first part of a 2-part series where we will discuss the basics of heart disease, the inherent risk factors underwriters assess, the methods for diagnosing CAD, and how an informed AgencyONE 100 Advisor and their clients can help to positively affect the outcome of their cases.
 Coronary Artery Disease (CAD) is still the #1 Killer in developed countries. While the past 30 years have seen remarkable advances in the diagnosis, treatment and prevention of coronary disease, the single most important factor in longevity and survivability is….your client.
Coronary Artery Disease (CAD) is still the #1 Killer in developed countries. While the past 30 years have seen remarkable advances in the diagnosis, treatment and prevention of coronary disease, the single most important factor in longevity and survivability is….your client.
A very scary fact is that often the first sign of heart disease in an otherwise healthy individual is DEATH. Life Insurance Underwriters look at ALL the risk factors when reviewing insurance case files. While some people are predisposed to developing coronary artery disease due to family history, most of the other risk factors are tied to individual behavior. Behaviors CAN BE MODIFIED and may result in SIGNIFICANT BENEFICIAL EFFECTS.
We all know that the heart is the engine that pumps blood to the entire body, but we often forget that the heart has its own blood supply provided by rather small coronary arteries. A narrowing of the blood flow through any of the coronary arteries can lead to a Heart Attack (MI—Myocardial Infarction) which literally means Heart Muscle Death.
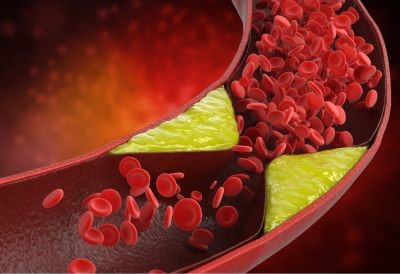 Cholesterol plaque buildup inside the coronary arteries is the culprit most of the time. This process can be slow to occur over decades. With people living longer, we are seeing more cases of previously undiagnosed coronary artery disease showing up with first-time symptoms in those over age 75.
Cholesterol plaque buildup inside the coronary arteries is the culprit most of the time. This process can be slow to occur over decades. With people living longer, we are seeing more cases of previously undiagnosed coronary artery disease showing up with first-time symptoms in those over age 75.
RISK FACTORS ASSESSED
Family History – The one risk factor that you cannot modify is your genes…at least not yet! However, knowing that you have a family prone to heart disease can provide you with the knowledge and hopefully the time to modify your lifestyle and delay or prevent coronary artery disease.
High Blood Pressure – This condition is pretty easy to control with the medication options available today.
Cholesterol and Triglycerides – A healthy diet and exercise is a good start. Statin and other medication options today have also reduced this mortality risk factor.
Obesity – Do your clients know their BMI (Body Mass Index)? A person with a BMI equal to or over 30 is considered obese. Accumulation of fat in your body generally also means accumulation of fat in your coronary arteries…. a true risk factor.
Diabetes – Coronary Artery Disease and Diabetes are mortality multipliers – meaning life expectancy is potentially lower and the underwriting risk is higher when these two are tied together. Tight control of A1C values in people with Diabetes will slow the progression of CAD. New oral medications and injectables are making a positive impact on controlling Diabetes and Obesity, thereby lowering the risks of death from Coronary Artery Disease.
DIAGNOSING CORONARY ARTERY DISEASE
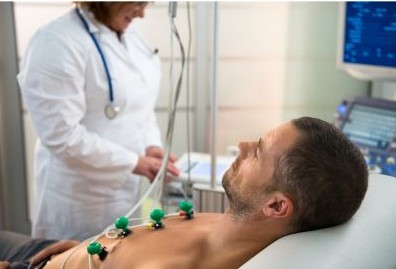 Resting EKG – This is the first line screening test. It is a simple test of electrical signals across the heart muscle. An abnormal EKG can lead to additional diagnostic testing as a resting EKG is really just a screening test. Life insurance companies have started to lean away from resting EKG requirements and are choosing a new blood test called NT-PRO BNP, a protein marker specific to the heart muscle. Elevations of this protein correlate with the heart working too hard.
Resting EKG – This is the first line screening test. It is a simple test of electrical signals across the heart muscle. An abnormal EKG can lead to additional diagnostic testing as a resting EKG is really just a screening test. Life insurance companies have started to lean away from resting EKG requirements and are choosing a new blood test called NT-PRO BNP, a protein marker specific to the heart muscle. Elevations of this protein correlate with the heart working too hard.
Stress Test/Stress EKG/Treadmill – This is still an excellent step 2 test to identify the presence of Coronary Artery Disease. A rising heart rate during exercise shows a disturbance in the normal electrical conduction system when that area of the heart does not receive enough oxygenated blood, usually due to the narrowing of the coronary artery blood flow. Stress tests are generally performed WITHOUT dye. However, the use of radioactive markers and dyes during testing can be visually diagnostic and show areas of perfusion issues and whether or not the heart muscle is getting enough oxygen – a possible indication of coronary blockage.
Echocardiogram/Stress Echocardiogram – While Echocardiograms are excellent tools for “seeing” how the heart muscle and valves are working, a Stress Echocardiogram is a valuable tool that searches for Coronary Artery Disease by looking at wall motion of the heart muscle during exercise. Lack of oxygen or coronary blockage shows up as lower or impaired wall motion dynamics.
Chest CT Scans/Coronary Calcium Scores/CT Angiogram – With just 10-15 minutes in the CT scanner, doctors can visualize those coronary arteries for cholesterol plaques and have an extremely good indication of the presence and extent of any coronary artery disease.
 Cardiac Catheterization – This is still considered the Gold Standard but there are risks associated with this course of action. Cardiac catheterization means threading a catheter into the coronary arteries and injecting dyes. This procedure affords the cardiologist the ability to treat Coronary Artery Disease with STENTS that open clogged arteries. Opening a narrow coronary artery with a stent can offer IMMEDIATE relief to the patient, return normal blood flow to that area of the heart, and often stop or prevent an infarction of muscle tissue.
Cardiac Catheterization – This is still considered the Gold Standard but there are risks associated with this course of action. Cardiac catheterization means threading a catheter into the coronary arteries and injecting dyes. This procedure affords the cardiologist the ability to treat Coronary Artery Disease with STENTS that open clogged arteries. Opening a narrow coronary artery with a stent can offer IMMEDIATE relief to the patient, return normal blood flow to that area of the heart, and often stop or prevent an infarction of muscle tissue.
CASE STUDY
Mr. Smith is 57 years old and recently had an Executive Physical exam with no symptoms. He is slightly overweight with a BMI of 36. The client had a routine “Total-Body” CT scan and posted a coronary calcium score of 144. A significant percentage of this is in the LEFT MAIN coronary artery. A follow up diagnostic test showed no major concerns from a cardiac standpoint.
The AgencyONE underwriting team and advisor discussed how the underwriting risk factors were going to be perceived by the carrier underwriters and how best to prepare Mr. Smith for the insurance exam and lab work. The client became actively engaged in the underwriting process and offered to go back to his cardiologist to specifically address some of the concerns that existed in the medical chart notes.
AgencyONE positioned Mr. Smith’s case with a carrier partner whose competitive guidelines for calcium scoring were in line with what we needed and negotiated a NON-SMOKER PLUS for $3.5 million in coverage.
Our next ONE Idea in April of this 2-part Coronary Artery Disease series, will take a deeper dive into CAD cases, discuss the medical and surgical management options we are seeing, and discuss more specifically the risks in underwriting Coronary Artery Disease.
As always, AgencyONE’s underwriting unit is here to answer your underwriting questions and help you better understand the diseases and risk factors underwriters assess. The more our AgencyONE 100 Advisors know, the easier it will be to prepare your clients for the underwriting process, and the more likely your case is to proceed smoothly and get placed at the right carrier for the best possible rate.
")
")
")